

Desort-Henin: The SAIVE Trial, Post-Exposure use of ivermectin in Covid-19 prevention: Efficacy and Safety Results
Desort-Henin, 399 patient ivermectin prophylaxis RCT: 96% fewer cases [p<0.0001]. PEP RCT 399 patients in Bulgaria showing significantly lower COVID-19 cases..
 c19ivm.org
c19ivm.org
Results
- Significantly lower COVID-19 cases with ivermectin prophylaxis.
- Significantly lower cases with high viral load.
- No participant had severe symptoms, required oxygen, or was hospitalized.
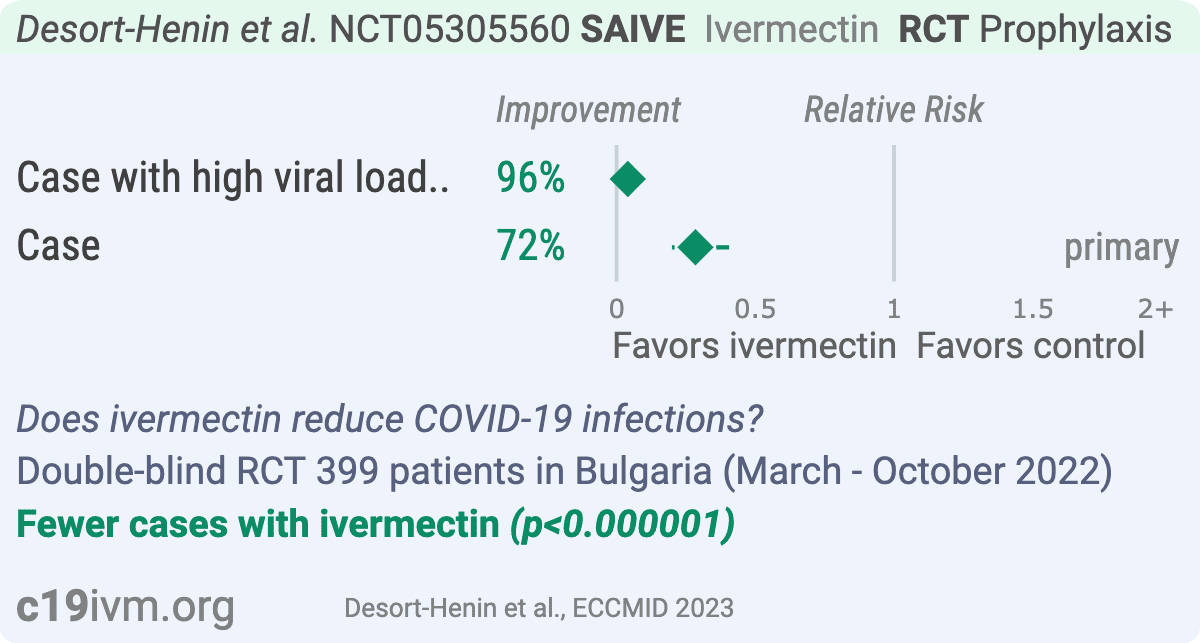
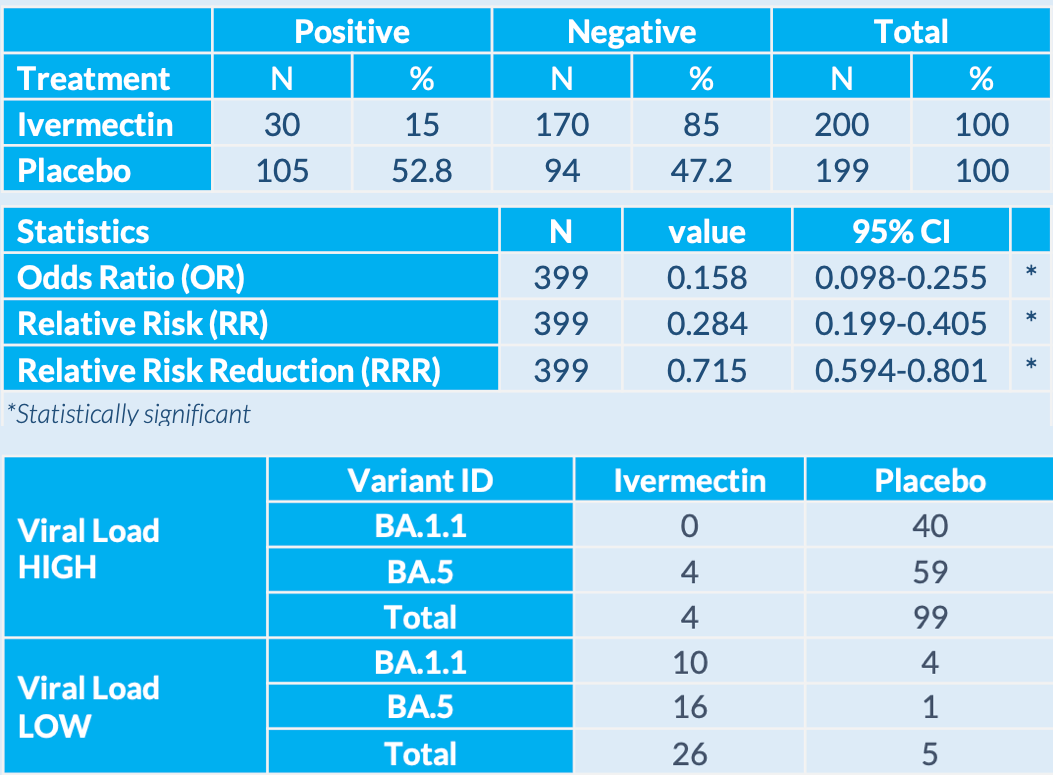
- Risk of case with high viral load, 96.0% lower, RR 0.04, p < 0.001, treatment 4 of 200 (2.0%), control 99 of 199 (49.7%), NNT 2.1.
- Risk of case, 71.6% lower, RR 0.28, p < 0.001, treatment 30 of 200 (15.0%), control 105 of 199 (52.8%), NNT 2.6, primary outcome.
3
This study demonstrated highly statistically significant evidence in a large, randomized, double-blind, placebo-controlled study that daily oral treatment with ivermectin reduced the risk of infection following exposure to SARS-CoV-2.
Ivermectin was also shown to be safe in doses and duration higher than currently used in approved indications.
Download available for when it is retracted and pulled from the journal servers:
Poster Saive April2023 Ok3
203KB ∙ PDF File
Download
A Study to Evaluate the Efficacy and Safety of Ivermectin in COVID-19 Prevention - Full Text View - ClinicalTrials.gov
A Study to Evaluate the Efficacy and Safety of Ivermectin in COVID-19 Prevention - Full Text View.
Here's a good write up on this study:

Ivermectin efficacy finally proven in ‘gold-standard’ RCT – Aldous
A RCT on Ivermectin efficacy for preventing and treating COVID-19 has been released, as discussed in this article by Prof Colleen Aldous.
 www.biznews.com
www.biznews.com
Large, well-designed randomised control study shows Ivermectin efficacy in preventing and treating COVID-19
By Colleen Aldous, Phillip Oldfield"Another large randomised control study on ivermectin efficacy for preventing and treating COVID-19 has been released to the public ahead of publication in an academic journal. But unlike negative results trials, there has not been a big international splash across the mainstream media coordinated by a large publicity agency such as Bell Pottinger. Why? Because the results are undeniably positive, showing the efficacy of ivermectin in reducing infection after exposure by 72%, documented in a press release on Jan 5 2023(1).
This is the best quality RCT we have yet seen published on ivermectin. It is called the SAIVE Trial (NCT 05305560)(2) and is part of MedinCell’s research supporting their development of a novel slow-release form of ivermectin. Although sparse results have been released so far, the quality of the study is apparent. A total of 399 unvaccinated participants completed the study as per the protocol. The number intended for treatment is not available yet, but I anticipate that the only difference would be that the ITT number for the control group may have been 200. Those participants who received daily oral ivermectin showed a 72% reduction in COVID-19 infection compared to the control group.
The study was carried out in Bulgaria between March and November last year when we saw a global reduction of SARS-COV2 infections and a decrease in the severity of COVID-19. Vaccination could have been a confounding factor in the results, but the inclusion criterion of being unvaccinated accounted for that. It was a multi-centre study, which shows replicability to some degree, a central tenet of good science. It was a parallel-group, double-blinded, randomised and placebo-controlled study. There is little that can be done to improve the rigour of this study design. It was also overseen by a U.S.-based independent Data Monitoring Committee to ensure compliance and provide further quality assurance. Participants were included in the study within five days after close exposure to somebody with a confirmed infection. This ensured very early treatment that some could consider prophylactic. The dosages were more than adequate, with daily doses of ivermectin taken orally at 200 microgram/kg on Day 1, followed by 100 microgram/kg daily from Day 2 to Day 28. This long-term daily dose design was likely to reflect future trials of MedinCell’s planned slow-release ivermectin injectable.
Of the 200 participants who received ivermectin, 30 showed laboratory-confirmed infections between Days 1 and 28 of the study. Of the 199 participants who received the placebo, 105 showed infections in the same period. For those who like Fisher’s p-value, this renders a p < 0,0001. There were no unexpected side effects, and safety and tolerability were once again demonstrated. Mortality data is not available, but this study occurred during the omicron infection period, where mortality was markedly reduced compared to the prior strains. MedinCell has undertaken to publish its results in a scientific journal in future. I am keen to see the details of when PCR tests in the patients across both groups came back as positive, how long before they were negative, symptom onset and symptom severity comparisons between the groups.
Looking at the history of research into ivermectin as a treatment for COVID-19, I can identify a few, amongst many, critical papers along with this latest research, where science has shown us a tool that could have saved millions of lives. To put it into a bullet story:
- Australian lab experiment of 2020(3): Prof Kylie Wagstaff, whose previous work showed that ivermectin is a specific inhibitor of importin α/β-mediated nuclear import and thus can inhibit replication of HIV-1 and dengue viruses, showed that ivermectin killed SARS-COV2 in the laboratory experiment. This experiment led to some doctors initially using ivermectin at the same dosages used for treating scabies. Some dismissed it as irrelevant because of the ivermectin concentrations used, but the experiment was a proof-of-concept study only, with no intention of reflecting dose responses.
- Zimbabwean blood oxygenation improvement paper of 2022(4): Dr Jackie Stone successfully treated patients on her regimen, which included ivermectin. For some patients, records of blood oxygenation had been kept from the start of treatment for several hours. She showed how quickly the blood oxygenation improved after the initiation of therapy. These results were also found in other studies in Nigeria and the US. This paper shows another possible mechanism of action for ivermectin in its success against the virus. Along with the repeated studies, the drug has an undeniable effect in SARS-COV-2 infected patients.
- Hemagglutination (blood clumping) paper of 2022: In another laboratory experiment, Boschi et al. (5) were able to explain why Dr Jackie Stone was able to show such an immediate response to ivermectin treatment. Using the Wuhan, Alpha, Delta and Omicron B.1.1.529 lineages of SARS-CoV-2 mixed with human red blood cells (RBCs), they showed that ivermectin prevented blood clumping when added to RBCs before infection and reversed it when added after infection. The earlier strains of COVID-19 were characterised by virus in the lungs, where its spike protein would cause RBCs to clump, thus reducing their capacity to carry oxygen and resulting in a fall in blood oxygenation levels. Omicron did not affect the lungs as badly. By reversing the blood clumping, oxygenation improved.
- MedinCell’s RCT(1) – yet to be published in an academic journal: This is the best RCT design yet to test ivermectin efficacy. Unvaccinated people exposed to people diagnosed with COVID-19 showed a much lower likelihood of contracting the illness after taking ivermectin. More than half of the placebo group got infected. Although the treatment protocol is different to other RCTS, testing a longer regimen following their further product development of a longer-acting ivermectin injectable, it shows a reduction in infection amongst people who had ivermectin post-exposure to a confirmed COVID-19 case.
Who employs multinational public relations, reputation management and marketing companies to put out the anti-ivermectin propaganda? Remember the FDA’s widely reported “You are not a horse. You are not a cow. Seriously, y’all. Stop it.” A slogan that became as well-known globally as the “It’s not inside, it’s on top” slogan in South Africa. The problem is that those in the know who are aware that ivermectin won its developers a Nobel Award for its human use could see through this propaganda immediately. Still, the general public is led to respect the utterings of authorities such as the FDA in the States, SAHPRA in South Africa and indeed the World Health Organisation (WHO) globally, and are taken in by this kind of mis- / dis-information.
Who controls what information is published in mainstream media and academic journals? The poor ivermectin studies, which showed an apparent ineffectiveness of ivermectin to treat COVID-19 received significant media airplay. But the studies that showed the positive results were not treated equally. In October 2022, we looked at all the published data on ivermectin and COVID-19 that we could find in PubMed. At that point, the totality of evidence leaned towards showing evidence for efficacy, with more studies showing efficacy or potential efficacy than those showing a lack of efficacy. The science is therefore being misrepresented in the mainstream media in favour of a skewed focus on the negative and gaslighting those studies showing efficacy. The TOGETHER Trial for ivermectin has several flaws, which many scientists across the globe responded to by writing letters to the editor of the New England Journal of Medicine (NEJM), but not one was published. In fact, they were returned stating that the journal had limited space etc., and one person on the editorial team went as far as publicly stating that no letters of concern about the trial were received! Trying to get anything positive about ivermectin published anywhere has become nearly impossible.
Why do so many people still follow the predominant and distorted narrative that ivermectin has no place in COVID-19 treatment in the face of all the evidence that it works? Some colleagues whom I respect still try and point out to me that my defence of ivermectin as a COVID-19 treatment is misplaced. I cannot determine why they cannot accept that science would involve looking at the totality of the evidence. Why do they dismiss all evidence that is not an RCT? Now, at last, there is an RCT that is appropriately designed that shows efficacy. Let’s see how many can change their thinking and understand that evidence-based medicine involves more research than RCTs. That laboratory studies can be used to explain clinical findings. That observational studies can provide good honest results that can be backed up by RCTs but are the first research to appear in a pandemic. While scientific scepticism is essential, adversarial dismissiveness has proven to be harmful.
..."
